






| Journal of Clinical Gynecology and Obstetrics, ISSN 1927-1271 print, 1927-128X online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Clin Gynecol Obstet and Elmer Press Inc |
| Journal website http://www.jcgo.org |
Case Report
Volume 4, Number 4, December 2015, pages 314-315
Intrapartum Diagnosis of Idiopathic Constriction Ring Dystocia
Shunji Suzukia, b, Sayuri Kondoa
aDepartment of Obstetrics and Gynecology, Japanese Red Cross Katsushika Maternity Hospital, Tokyo, Japan
bCorresponding Author: Shunji Suzuki, Department of Obstetrics and Gynecology, Japanese Red Cross Katsushika Maternity Hospital, 5-11-12 Tateishi, Katsushika-ku, Tokyo 124-0012, Japan
Manuscript accepted for publication December 07, 2015
Short title: Constriction Ring Dystocia
doi: http://dx.doi.org/10.14740/jcgo380e
| Abstract | ▴Top |
We present here a case of idiopathic constriction ring dystocia. In the case, an intrapartum ultrasonography showed a thickening of the anterior wall of the uterus during labor. Cesarean section identified the constriction ring of the uterine myometrium strangling the fetal neck at 3 - 4 cm above the Bandl’s contraction ring.
Keywords: Constriction ring; Dystocia; Bandl’s contraction ring; Ultrasonography
| Introduction | ▴Top |
Obstructed labor or labor dystocia is a common emergency in obstetrics; however, dystocia due to uterine rings is a rare phenomenon. A constriction ring has been reported to be a localized tetany of the uterus that occurs in prolonged labor with rupture of the membranes [1]. It is usually localized to a thickened area of the myometrium over a point of fetal body or at a level just below it [1-3]. Therefore, it is differentiated from the Bandl’s contraction ring (also known as pathological retraction ring) which is the abnormal junction between the two segments of the human uterus and also associated with the dysfunctional and prolonged labor or fetal head malposition [1, 4, 5]. Recently, some cases of ultrasonographic observation of Bandl’s contraction ring have been reported [4, 5]. In these cases, a thickening of the anterior wall of the uterus has been detected at the level of the lower uterine segment [4, 5]. We present here a case of constriction ring dystocia. In the case, an intrapartum ultrasonography showed a thickening of the anterior wall of the uterus during labor at above the Bandl’s contraction ring.
| Case Report | ▴Top |
A 32-year-old parous (gravida 2, para 1) Japanese woman at 38 weeks was admitted at our hospital in labor following premature rupture of the membranes. She delivered a healthy female baby weighing 3,312 g (Apgars 9/10) without any obstetric problems at 30 years old. At admission, she was in active labor with regular contractions of the uterus occurring every 2 - 3 min. Examination revealed advanced cervical dilatation, effacement, but high station (5 cm/80%/-3) during the interval of the labor pains. During the acme phase of the labor pains, the fetal head was lifted to the higher station (-4 to -5). An ultrasound evaluation identified occipito-posterior presentation of the fetus and oligohydramnion (amniotic fluid index: 1 cm). A thickening of the anterior wall of the uterus was detected between the fetal head (jaw) and shoulder (Fig. 1). The size and shape of the ring were unaffected by contractions. Dystocia due to constriction ring or contraction ring (Bandl’s contraction ring) was suspected. Possible interventions including tocolysis using nitroglycerin or magnesium sulfate were discussed with the patient, and she selected a cesarean delivery. A female infant weighing 2,834 g with Apgars 9/9 was delivered by cesarean section. Surgeons identified the constriction ring of the uterine myometrium strangling the fetal neck at 3 - 4 cm above the Bandl’s contraction ring (Fig. 2). After the deliveries of the fetus and the placenta, the constriction ring disappeared. There was no intrauterine septum or synechia. Her puerperium was uncomplicated.
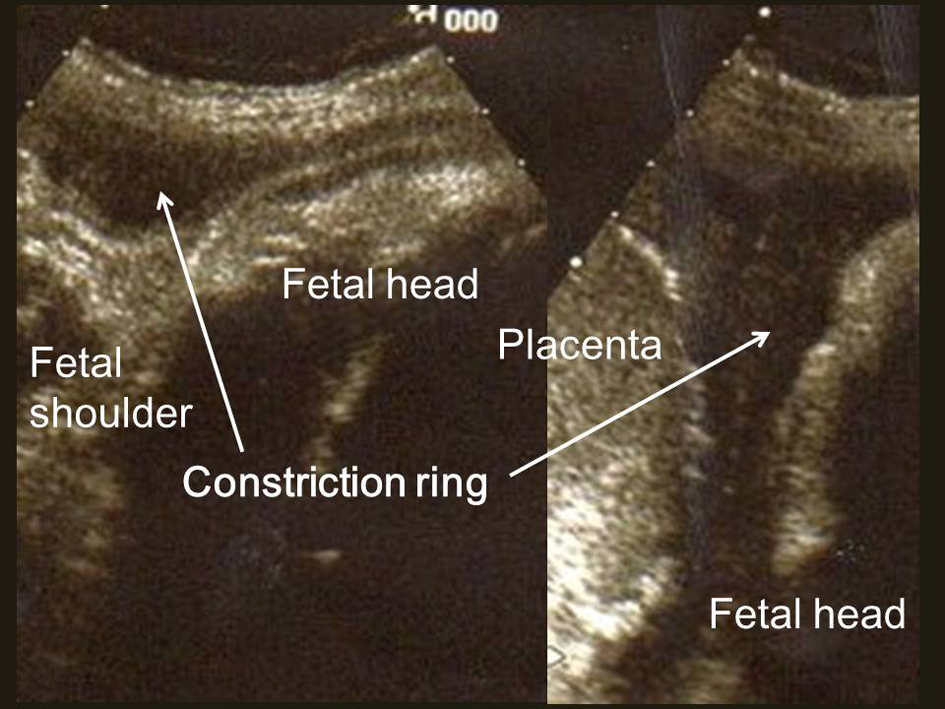 Click for large image | Figure 1. Ultrasonographic view of the uterine constriction ring (arrow) in a case of obstructed labor. |
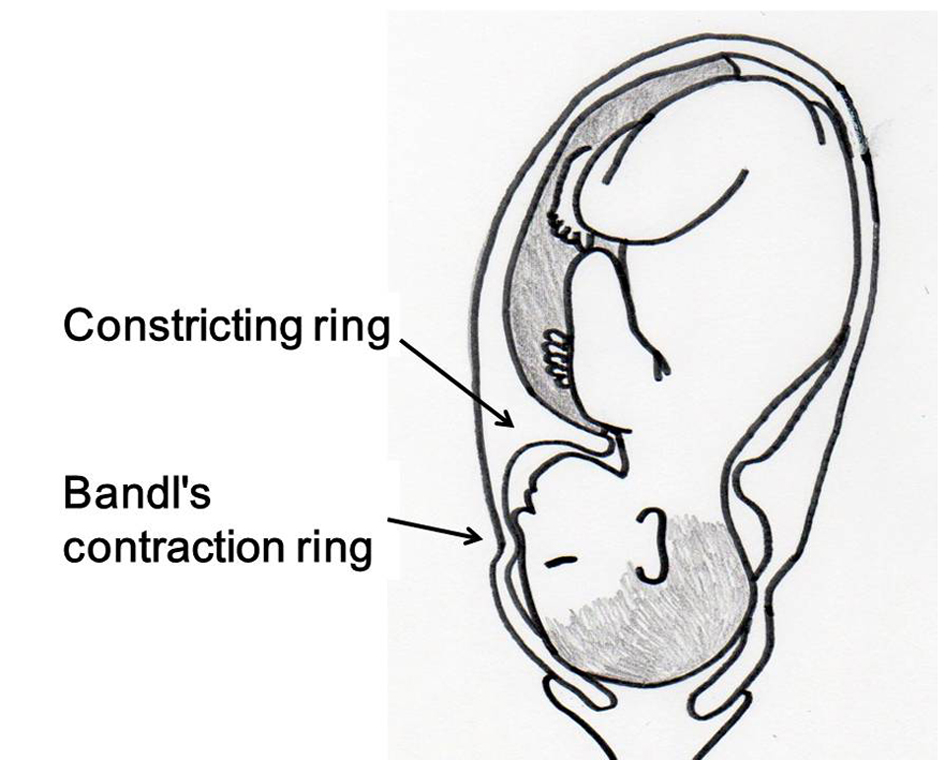 Click for large image | Figure 2. Constriction ring around the fetal neck in a case of obstructed labor. |
| Discussion | ▴Top |
The occurrence of constriction ring will be one of the causes of maternal near miss and unexpected obstructed labor.
To date, the reports of the ultrasonographic observation of constriction ring dystocia have been rare. In the current case, the position of the ring was observed to be at above that of Bandl’s contraction ring; however, the thickened myometrium appearing as a homogeneous layer between the serosa and the decidua in the constriction ring by ultrasonography seemed to be very similar to that of Bandl’s contraction ring reported previously [1, 4, 5]. In this case, however, no thinning of the lower uterine segment was observed at the time of cesarean. The thickness of the uterine wall above and below the ring seemed to be approximately equal [1]. This finding may be different from that in Bandl’s contraction ring associated with excessive thinning of the lower uterine segment leading to the increased risk of uterine rupture. Unfortunately, in this case we did not check this point by ultrasonography; however, this may be one of the differential points in the ultrasonographic examination for the management of the two types of ring dystocia. If we had diagnosed this case as constriction ring dystocia clearly, we may have a possibility to recommend tocolysis strongly on the informed consent.
This may be the first observation of the changes in station of the fetal head during obstructed labor due to constriction ring. If the fetus is strangulated by the uterus during labor, the fetus may be lifted during the acme phase of the labor pains. To date, the pathogenesis of constriction ring dystocia has not been well documented. In this study, some possible conditions associated with the mechanisms leading to the occurrence of constriction ring dystocia can be proposed such as occipito-posterior presentation of the fetus and oligohydramnion [1]. The elucidation of the pathogenesis and accurate diagnostic methods of constriction ring dystocia is needed by accumulation of the same case reports.
Grant Support
This study received no funding.
Conflict of Interest
The authors declare that they have no conflict of interest.
| References | ▴Top |
- Greenhill JP. Constriction ring dystocia. In: Greenhill JP (ed) Obstetrics. Asian ed. 13th ed. Igaku Shoin Ltd., Tokyo & Osaka, 1965, pp 838-839.
- Jeanty P, Johns R, Boehm F. Uterine ring and fetal demise. J Ultrasound Med. 1989;8(11):635-638.
pubmed - Kaye CH. Constriction ring dystocia. Can Med Assoc J. 1974;110(5):535-538.
doi - Buhimschi CS, Buhimschi IA, Weiner CP. Ultrasonographic observation of Bandl's contraction ring. Int J Gynaecol Obstet. 2004;86(1):35-36.
doi pubmed - Tinelli A, Di Renzo GC, Malvasi A. The intrapartum ultrasonographic detection of the Bandl ring as a marker of dystocia. Int J Gynaecol Obstet. 2015 in press.
doi pubmed
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Clinical Gynecology and Obstetrics is published by Elmer Press Inc.