






| Journal of Clinical Gynecology and Obstetrics, ISSN 1927-1271 print, 1927-128X online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Clin Gynecol Obstet and Elmer Press Inc |
| Journal website http://www.jcgo.org |
Original Article
Volume 3, Number 4, December 2014, pages 129-132
The Utility of Microsurgical Loupes in Performing Colposcopy: A Pilot Study
Emily E. Hadleya, Virginia A. Rautha, Ana M. Rodrigueza, Mostafa A. Borahaya, Kristofer Jenningsb, Pooja R. Patela, c
aDepartment of Obstetrics and Gynecology, The University of Texas Medical Branch in Galveston, TX, USA
bDepartment of Biostatistics, The University of Texas Medical Branch in Galveston, TX, USA
cCorresponding Author: Pooja R. Patel, Department of Obstetrics and Gynecology, The University of Texas Medical Branch, 301 University Boulevard, Galveston, TX 77555-0587, USA
Manuscript accepted for publication October 17, 2014
Short title: Microsurgical Loupes in Colposcopy
doi: http://dx.doi.org/10.14740/jcgo291w
| Abstract | ▴Top |
Background: The aim of the study was to compare microsurgical loupes to traditional colposcopes with regard to physician comfort, efficiency and accuracy in performing colposcopy.
Methods: This was a prospective cohort study. Colposcopy was performed using microsurgical loupes and traditional colposcopes on the same set of patients. Time to completion, biopsies to be taken, and comfort level associated with examination for each method were recorded.
Results: A total of 54 patients were included in this study. It took significantly less time to evaluate the cervix with loupes (mean: 72.4 ± 39.7 seconds) compared to the colposcope (102.3 ± 48.9 seconds; P < 0.001). The comfort level for using loupes was better than that for colposcopes (2.8 ± 2.4 vs. 5.7 ± 2.8, respectively; P < 0.001). The probability that the lesions to be biopsied matched for both modalities was 0.90 (95% CI: 0.81 - 0.95).
Conclusions: Microsurgical loupes have comparable accuracy to traditional colposcopes, but with shorter exam time and better comfort for the provider.
Keywords: Colposcopy; Cervical dysplasia; Cervical cancer screening
| Introduction | ▴Top |
Colposcopy is the diagnostic procedure used to evaluate the cervix after abnormal findings on a Pap test. Since the mid-1900s, this has traditionally been performed using a colposcope, a large microscope that is used by the provider to examine magnified views of the cervix. This instrument however is expensive, difficult to transport, and cumbersome to manipulate [1, 2]. The cost-effectiveness and applicability of this large device is, therefore, limited in third-world countries where its need is the greatest [3]. Current studies show that colposcopy is associated with significant anxiety as it pertains to the workup of precancerous lesions [4, 5]. Therefore, finding a method that decreases time to evaluate the cervix may ameliorate the anxiety associated with the procedure. Alternatives including digital colposcopic instruments have been evaluated to overcome these shortcomings of the traditional colposcope; however, these require up-to-date technology and are expensive, again limiting use in developing countries [6]. Microsurgical loupes, glasses with telescopic lenses that allow for comfortable magnification of visual fields, may better serve as such an alternative due to lower costs, better ergonomics, and easier transportability (Fig. 1). In this study, we compare microsurgical loupes to traditional colposcopes with regard to physician comfort, efficiency as well as accuracy in performing colposcopy.
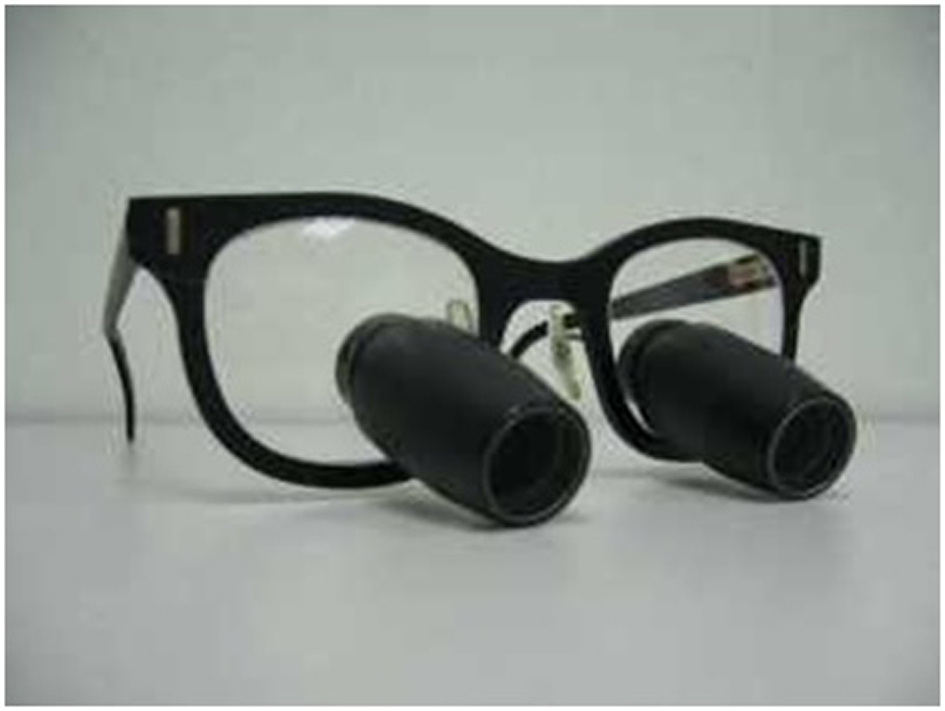 Figure 1. Microsurgical loupes are used routinely for magnification during surgical and dental procedures. Figure 1. Microsurgical loupes are used routinely for magnification during surgical and dental procedures. |
| Methods | ▴Top |
After Institutional Review Board approval was obtained, female inmates of the Texas Department or Corrections who presented to the Carol Young Medical Facility in Texas City, Texas and patients who presented to the Dysplasia and Cancer Stop Clinic at the University of Texas Medical Branch’s Regional Maternal and Child Health Program in McAllen, Texas for colposcopy were offered participation in the study. After obtaining consent, a routine gynecologic exam was performed in preparation for colposcopy. After placement of the speculum, 5% acetic acid was applied to the cervix. Half the patients underwent examination with the traditional colposcope first while the other half underwent examination with the microsurgical loupes first (randomly assigned). The duration of each inspection method was recorded as well as biopsies that the provider would take based on visualization by that method. Finally, the provider graded the comfort level with each inspection method on a scale of 1 - 10 (1 being the most comfortable and 10 being the least comfortable).
A total of three gynecologists collected data for this study. Microsurgical loupes were donated by Design for Vision, Inc., custom-fit for each gynecologist. All microsurgical loupes had eye-pieces with × 6 magnification. A standard Seiler 935 colposcope (Seiler Instrument Inc., St. Louis, MO, USA) with × 7 and × 17 magnifications was used for the traditional colposcopy.
With regard to statistical analysis, time to completion and comfort of evaluation for each of the two methods were compared using a paired Wilcoxin test. The confidence interval (CI) for agreement in biopsies to be taken was generated using standard normal techniques (with continuity correction) for inference on proportions.
| Results | ▴Top |
A total of 54 examinations were completed for this study using both modalities of evaluation. Gynecologist A examined 12 patients, gynecologist B examined 17 patients, and gynecologist C examined 25 patients. The distribution of indications for colposcopy, race and age are depicted in Table 1.
| Table 1. Demographic Data |
It took significantly less time to evaluate the cervix with loupes (mean: 72.4 ± 39.7 s) compared to the colposcope (102.3 ± 48.9 s; P < 0.001). The comfort level for using loupes was better than that for colposcopes (2.8 ± 2.4 vs. 5.7 ± 2.8, respectively; P < 0.001). The probability that the lesions worthy of biopsy matched for both modalities was 0.90 (95% CI: 0.81 - 0.95). This analysis is summarized in Table 2.
| Table 2. Comparison of Outcomes for Loupes Versus Traditional Colposcope |
| Discussion | ▴Top |
Our study shows that microsurgical loupes may be a feasible alternative for colposcopy. This has profound implications for use, especially in developing countries where the need for colposcopy is greatest. The use of loupes for colposcopy provides a more portable and cheaper method than traditional colposcopes, two traits that would make this attractive for use in developing nations. Colposcopes range from $4,000 to $10,000 US dollars, whereas loupes are a couple hundred US dollars. In addition, the providers in the study reported better ergonomics for the physician in the use of loupes. It was much easier to manipulate the loupes as the physician simply had to adjust her head instead of having to battle moving the colposcope to focus on the cervix. One of the most difficult parts about the loupes was the adjustment of the light source, as we used a stand-alone light for the light source while using the loupes. The key for this was to place the examiner’s head and loupes in the same plane as the light source, so that the light was shining from the same angle as the position of the provider’s head. Once this routine was perfected, the light source was no longer a weakness. However, further research should be done into determining if a portable light source can be attached to the loupes headpiece.
The providers in this study felt that × 6 magnification was adequate for evaluation of the cervix. The original colposcope developed by Hinselman in the 1920s provided illuminated magnification ranging from × 6 to × 40. We were surprisingly unable to find any studies that examined the minimal amount of magnification needed for accurate evaluation of the cervix. We did come across a study from 1993 that evaluated × 5 loupes as an adjunct to Pap tests for cervical cancer screening [7]. However, this study was based on the assumption that colposcopy was the gold standard for evaluation. Interestingly, of 189 women that were found to have negative Pap tests and no lesions on colposcopy, 10 of these women were found to have lesions on the examination by the × 5 loupes, suggesting that the × 5 loupes provided some sort of visualization that the colposcope did not. We came across another study that confirmed the utility of evaluation by Aviscope®, a handheld × 4.5 magnification device, as a screening test [8]. Again, this study assumed colposcopy was the gold standard for evaluation of abnormal screening, and therefore compared evaluation by Aviscope to definite findings on colposcopy, as the intention was to find a screening method and not to compare findings to the traditional colposcope. In this study, of the patients with negative colposcopy (as per the traditional colposcope), approximately 20% had findings on exam by the Aviscope®, suggesting that visualization is possible at low magnification. We were able to find a two-part study from 1997 comparing loupes to colposcopes not as a screening tool, but as an instrument used to perform colposcopy. Although this study showed that loupes are adequate to perform colposcopy, it did not evaluate physician comfort and time to evaluate cervix [9, 10].
It would be unethical to compare the biopsies obtained from examination by loupe examination versus biopsies obtained from colposcope examination, as the colposcope is currently considered the gold standard. However, our study shows that cervical lesions suspicious enough for biopsy were very accurate. A total of five exams had extra lesions that showed up on the colposcope examination and did not show up on the loupes examination. Of these four were done to evaluate either LSIL or ASCUS/HPV+ Pap tests and one was done to evaluate the cervix post-LEEP. All of these non-concordant biopsies came back as CIN 1 or HPV-associated changes, suggesting that any discrepancies between the two modes of examination did not affect treatment outcome.
The main disadvantages associated with the loupes were the lack of an attached light source and the lack of a green filter. However, despite these shortcomings, the lesions to be biopsied matched remarkably well for both modalities.
Finally our study also supports the hypothesis that examination with loupes takes almost half the time than examination with colposcope. This may be critical in decreasing the anxiety associated with colposcopy, an effect that is well-documented in the literature. Both the patients and physicians would benefit from a method requiring shorter time for evaluation.
There are a few limitations to our study. First, because of the nature of the study, it was very difficult to blind the physician from results of each route of examination. As such, the second route of inspection for each patient may have been biased by the results of the first route. Second, we were unable to have higher magnification loupes as the higher the magnification, the longer and heavier the eye-piece. Nevertheless, given the high probability of lesions matching from both modalities of examination, this may be a moot point.
In conclusion, microsurgical loupes are comparable to traditional colposcopes. This allows providers a more ergonomic option for colposcopy that is more transportable and cheaper to utilize, two qualities critical to successful colposcopy in developing countries. Further research is needed into determining whether a green filter and/or attached light source would be useful.
Conflict of Interest
The authors report no conflict of interest.
| References | ▴Top |
- Kim YT, Kim JW, Kim SH, Kim YR, Kim JH, Yoon BS, Park YW. Clinical usefulness of cervicogram as a primary screening test for cervical neoplasia. Yonsei Med J. 2005;46(2):213-220.
doi pubmed - Stafl A. Cervicography: a new method for cervical cancer detection. Am J Obstet Gynecol. 1981;139(7):815-825.
pubmed - van Niekerk WA, Dunton CJ, Richart RM, Hilgarth M, Kato H, Kaufman RH, Mango LJ, et al. Colposcopy, cervicography, speculoscopy and endoscopy. International Academy of Cytology Task Force summary. Diagnostic Cytology Towards the 21st Century: An International Expert Conference and Tutorial. Acta Cytol. 1998;42(1):33-49.
doi pubmed - Kola S, Walsh JC. Determinants of pre-procedural state anxiety and negative affect in first-time colposcopy patients: implications for intervention. Eur J Cancer Care (Engl). 2012;21(4):469-476.
doi pubmed - Kola S, Walsh JC. Patients' psychological reactions to colposcopy and LLETZ treatment for cervical intraepithelial neoplasia. Eur J Obstet Gynecol Reprod Biol. 2009;146(1):96-99.
doi pubmed - Benavides J, Chang S, Park S, Richards-Kortum R, Mackinnon N, Macaulay C, Milbourne A, et al. Multispectral digital colposcopy for in vivo detection of cervical cancer. Opt Express. 2003;11(10):1223-1236.
doi pubmed - Mann W, Lonky N, Massad S, Scotti R, Blanco J, Vasilev S. Papanicolaou smear screening augmented by a magnified chemiluminescent exam. Int J Gynaecol Obstet. 1993;43(3):289-296.
doi - Denny L, Kuhn L, Pollack A, Wright TC, Jr. Direct visual inspection for cervical cancer screening: an analysis of factors influencing test performance. Cancer. 2002;94(6):1699-1707.
doi pubmed - Reed, TP, et al. Comparison of Standard and Loupe Colposcopy (Part I). Journal of Lower Genital Tract Disease. 1997;1(2).
- Reed, TP, et al. Comparison of Standard and Loupe Colposcopy (Part II): Initial Experience with a New 6x-10x Surgical Loupe. Journal of Lower Genital Tract Disease. 1997;1(2).
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Clinical Gynecology and Obstetrics is published by Elmer Press Inc.